The problem has been addressed by the Affordable Care Act, but the ACA is far from ideal. It still doesn't cover everyone, doesn't provide preventative care, and the ACA continues to involve inefficient private health insurance companies.
Private, for-profit insurance companies extract administrative and profit dollars well in excess of the 3% of total costs spent by government-administered health insurance. The Senate Commerce Committee reported in 2010 that in the individual health care market, the largest health insurers spent on average more than 26 cents out of every premium dollar on administrative costs and profits.
Under the ACA, new medical-loss-ratio floors went into effect on January 1, 2011. Health insurers will be required to spend no more than 20 cents out of every premium dollar for administration and profit in the individual and small-group markets, and no more than 15 cents in the large-group market. Thus, additional costs for administration and profit will unnecessarily absorb a minimum of 13% of the premiums paid to private insurers under the ACA, compared with government-run plans.
Our uniquely American employer-provided health insurance hurts our competitiveness abroad. And those health insurance premiums make it more profitable for companies which want to expand domestic production to buy machines and otherwise automate, instead of hiring new employees.
Michael Moore's documentary film, Sicko, shows us, to our embarassment, superior health care systems in foreign countries. Here is a description of the government-run health insurance program in Canada. And here's another. It works, everyone's covered, it costs half as much as ours, and Canadians live two years longer than we do.
Our government already provides a major share of our health insurance. Federal, state, and local spending on health care totals about $1.065 trillion annually, or about 46% of total health care spending. (Private insurance companies pay 36%, with most of the rest coming from direct patient payments.) It makes sense to extend this existing government capability to the currently uninsured and those covered by employer-based plans.
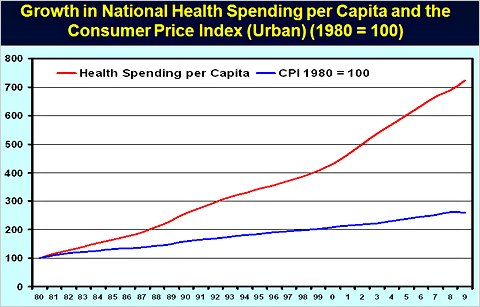
The cost of health care has been rising much more rapidly than other prices, as shown by the following chart. This means that, unless corrective action is taken, health insurance will consume an increasing portion of our federal budget, and increasingly contribute to our national debt.
If we work together, we can almost certainly further reduce our total health care expense dramatically. This is a golden opportunity to both reduce the national debt and, at the same time, provide good insurance coverage at an affordable price for everyone.
One essential goal is containment of national health care costs. The ACA provides for an Independent Payment Advisory Board to rein in costs. This would include costs now paid for ineffective procedures and costs now paid for excessive care, prescribed not as a defense against malpractice law suits, but because of financial considerations. Doctors and hospitals are currently paid for just about anything a doctor recommends. Yes, doctors and hospital administrators are humans, too.
The Public Option and Local Alternatives
And then there's the "public option," the government-run insurance alternative which was left out of the Affordable Care Act. At a meeting of the nation’s governors at the White House on February 28, 3022, President Obama signaled willingness to support Oregon U.S. Senator Ron Wyden's amendment to the ACA. This amendment would advance the date on which states can propose local alternatives to ACA by three years, from 2017 to 2014, when major elements of ACA take effect. It would allow individual states or regional alliances of states to design plans that avoid the individual private insurance mandate and the fines for employers who don't provide coverage. In fact, it would allow for states to implement single-payer systems, which Obama initially said was necessary “to keep the insurance companies honest.”
According to the Oregonian, under Sen. Wyden's bill, which is cosponsored by Republican Sen. Scott Brown of Massachusetts, states would be free to design health insurance programs that fit local needs and political standards as long as the result provides care to the same number - or more - people, contains costs and offers services that are equal to or better than those required in the 2010 ACA law.
It appears certain that Vermont will apply for a waiver: Vermont Senator Bernie Sanders told Ezra Klein of Daily Kos that:
“We believe Vermont stands a chance to be the first state in the nation to pass single-payer. The [newly elected Governor Peter Shumlin] campaigned on it, and we have support in the House and Senate. We're not asking for one nickel more than we'd otherwise get.”
On May 16, 2011, Vermont Governor Shumlin signed the ground-greaking single-payer plan into law. Gov. Shumlin was interviewed by Amy Goodman and Juan Gonzales of Democracy Now! on January 21, 2011, where he emphasized the cost-containment benefits and the groundwork he has laid to enact a single-payer health insurance system in Vermont. It can become a model for many other states, or even a national insurance program.
In Oregon, HB 3510 and SB 888 are bills entered into the state legislature establishing the Affordable Health Care for All Oregon Act, a single-payer program. The bills appear to have died in committee this year, and they will have to be resubmitted in 2012. They deserve our attention.
At the same time, Oregon's Gov. John Kitzhaber is proposing the establishment of "coordinated care organizations" (CCR's) to serve participants in the Oregon Health Plan, which is Oregon's Medicaid plan. Kitzhaber, a former emergency room physician, is promoting this revolutionary plan to both reduce costs and improve outcomes. Based on a successful trial program in central Oregon, the CCR's will provide comprehensive, one-stop, total health care, including preventive care. Here is an editorial report.
Gov. Kitzhaber was at the White House when President Obama said he supported Sen. Wyden's amendment to the ACA. Kitzhaber told Oregon Public Broadcasting. “I was at the White House when the President made that announcement and we feel it’s very, very good news for Oregon.”
But, again, our support is needed.
There have been recent, explosive increases in private insurance premiums of 20% to 45% for individuals and small businesses. The opportunity to create local responses to this threat, as exemplified by Vermont and Oregon, could help spur adoption of Wyden’s bipartisan approach.
Universal, low-cost health insurance would be a boon to both consumers and businesses. It would prove once again that government can really help us. And it would enhance chances for Obama's re-election.
Republicans in the House of Representatives have voted to repeal the Affordable Care Act. But one of the top Republican candidates for president dismayed the conservative political base by signing a health insurance law similar to the ACA while he was governor of Massachusetts. Here is a humorous article by The Onion, spoofing Mitt Romney apologizing for the political "liability" of trying to help his constituents.
Eliminating Medicare
Medicare for All is the generic title for universal, low-cost health insurance. But even Medicare itself is under attack. Who will insure seniors, if we don't have Medicare? According to this history of Medicare, only 13% of the elderly had health insurance when Medicare was enacted in 1965. Why? Old people were long considered "bad risks" by commercial insurers, and unions had not made much headway in obtaining coverage for retired workers through employer-sponsored plans.
But the Republican deficit reduction budget, adopted by the U.S. House of Representatives on April 15, 2011, will take us back to the old days. It privatizes Medicare, starting in 2021. Under this plan, those newly eligible for Medicare in 2021 would be given a voucher which they could use to help buy private health insurance policies. The problem is that the value of the vouchers would be indexed to the Consumer Price Index, rather than the average cost of health insurance policies.
Assuming that seniors would even be able to find companies that would insure them, it is likely that the cost of health insurance would continue to increase faster than the CPI (per the above chart). They would thus have to pay an ever-increasing share of health costs out of their own pockets, virtually eliminating Medicare as a defined benefit plan. Here is an analysis by Princeton economics professor Uwe E. Reinhardt, describing the harm caused by shifting many trillions of dollars back onto the elderly.
And here are are interactive maps prepared by Democrats on the House Committee on Energy and Commerce, which give access to details for each Congressional District of the Republican plan to reduce Medicare and Medicaid expenses.
As this is written in mid-2011, the Republican plan has proven widely unpopular. Their response is share their political misery by demanding that Democrats vote for cuts to Medicare in exchange for Republican votes to raise the national debt ceiling
Our own Republican Rep. Greg Walden, tried to minimize our reaction to the Republican Medicare plan in his April 18, 2011, constituent newsletter. Here's what Rep. Walden said:
I think you deserve a fact-based conversation on the budget. And the facts are, our budget does not propose any changes to Medicare or Social Security benefits for those 55 or older. Therefore, this plan will not cause you, as a Medicare and Social Security beneficiary, to lose service to your current doctor, prescriptions or pharmacy, and your Social Security benefits will not change.
We feel insulted to be told that those of us aged 55 and older should not be concerned with the Republican plan, since we are exempted from it. As involved citizens, we have every responsibility and intent to preserve the Medicare program for all those who follow us!
Raising Medicare Eligibility Age
Several major deficit-reduction proposals include raising Medicare’s age of eligibility to 67, as a way of improving Medicare’s solvency. But this study by the Kaiser Family Foundation indicates that this would raise the cost of health insurance for everyone.